
The Hidden Cost of Inefficient Radiology Workflows: What the Numbers Actually Show
Clinical Efficiency in Radiology: Why Radiology Workflow Optimization—and Display Calibration—Is a Quality Issue, Not a Cost Issue
The busiest quarter of your career probably isn’t behind you — it’s likely ahead.
Between 2018 and early 2024, radiology exam case loads grew by roughly 31%. That’s nearly 5% per year. The radiologist workforce, however, grew at a much slower pace. As a result, the added volume wasn’t shared evenly across the field. In fact, the top quarter of radiologists saw their daily caseload jump from about 57 studies to nearly 74 per day. On top of that, they worked 20% more clinical shifts per quarter than they did six years ago. [1]
Importance of Radiology Workflow Optimization

If you’ve felt the pressure, you’re not imagining it. And if you’re a practice administrator trying to figure out why throughput is stalling even as your team is working harder, the answer usually isn’t the radiologists — it’s everything around them.
The Swivel-Chair Problem
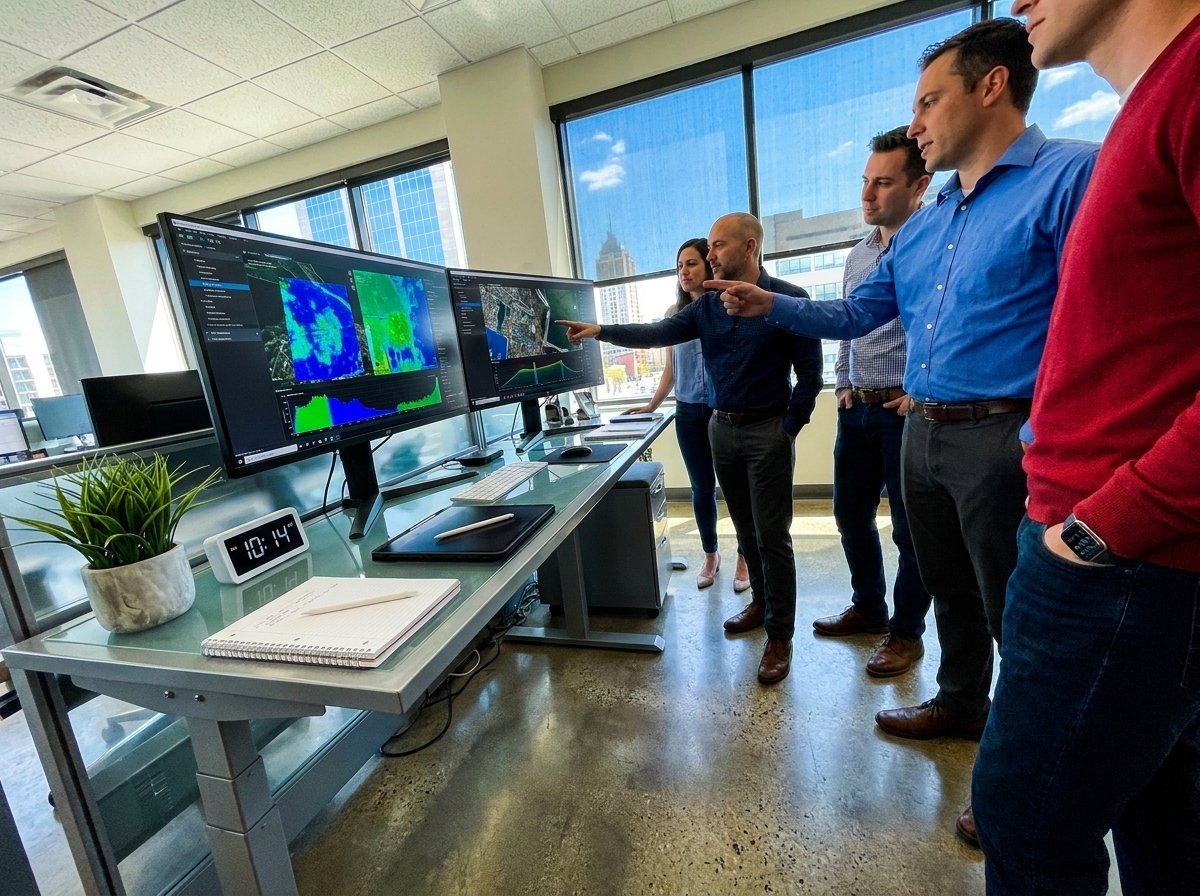
In a typical radiology department, a radiologist doesn’t just read studies. They log into one system to access the worklist. Then they switch to another to view images. After that, they use a third to write reports, and sometimes a fourth to message referring physicians. Industry analysts have called this the ‘swivel-chair problem’ — named for the act of rotating between multiple workstations to complete a single case. [2]
None of those transitions require clinical judgment. They require time, focus, and mental effort that could be spent on the scan. When you multiply each context switch across 50 or 70 cases a day, the total cost adds up fast — and none of it shows up on a productivity report.
Administrative Overhead Is a Clinical Problem
The link between admin work and diagnostic quality isn’t just theoretical. A review published in PMC found that burnout in radiology — which now affects more than 50% of physicians in the field [3] — is directly tied to more medical errors, higher malpractice risk, and worse patient outcomes. [4]
Radiology ranks highest in mental demand among all physician specialties. [5] So when that mental load is made worse by documentation tasks, billing steps, report formatting, and prior authorization work that has nothing to do with reading images, the risk to quality becomes real — not theoretical.
A Philips study surveying radiology staff across the U.S., UK, Germany, and France found that 44% of U.S. imaging technologists reported moderate to severe job stress. Poor technology and heavy workloads were the top causes. Even more telling: in the U.S., imaging directors were underestimating the burnout felt by their own staff — a gap that makes real change harder to drive. [6]
The Bottleneck Isn’t the Read | Radiology Workflow Optimization
Radiology practice leaders often treat capacity issues as a volume problem in radiology workflow optimization. They’re not entirely wrong — imaging demand is set to grow another 3–4% per year for the foreseeable future. That growth is driven by an aging population, more chronic disease, and wider use of advanced imaging. [7]
But there’s a second layer to the volume problem that doesn’t get enough attention. It’s the share of each radiologist’s day spent on tasks that aren’t reading. Answering phones, entering billing codes, using disconnected systems, completing paperwork for compliance rather than care — each of these is time that can’t be recovered.
The ACR has been clear on this point: cutting admin work — answering phones, calling in reports, completing billing paperwork — is one of the most effective ways to help practices manage volume without burning out their staff. [5]
What Efficient Workflow Actually Looks Like
Good radiology workflow optimization doesn’t mean faster reads under more pressure. Instead, it means removing the friction around the read. That way, the radiologist can focus on the work they were trained to do — with fewer interruptions and more support.
In practice, that means a single platform that connects imaging, reporting, and workflow in one place. It means smart case sorting so urgent studies come up first. It means structured reporting that captures what’s needed without adding extra steps in radiology workflow optimization. And it means clear data on turnaround times so practice leaders can spot problems before they grow.
When Carolina Radiology Associates moved from seven separate workstations to one connected platform, their CEO said it transformed their operation almost immediately. [2] That’s not a technology story — it’s a workflow story.
The Cost of Waiting | Radiology Workflow Optimization
Practices that fix radiology workflow optimization problems now will be better placed for the volume increases ahead. Those who wait will absorb the cost in one of three ways: staff burnout and turnover, errors from overloaded radiologists, or backlogs that limit patient access to timely imaging.
None of those outcomes are acceptable. And none of them are inevitable.
Qubyx was built to solve the specific Radiology Workflow Optimization challenges that radiology practices face — not as a generic healthcare IT platform, but as a system designed around the radiologist’s workflow. Learn how Qubyx addresses these friction points →
References
-
[1] Radiology Business. ‘Imaging volumes continue rising, but not all radiologists shouldering the same burden.’ January 2026.
-
[2] Intelerad. ‘Lightening the Load: How to Alleviate Radiologist Burnout.’ September 2024.
-
[3] PMC / National Institutes of Health. ‘Incidence and factors associated with burnout in radiologists: A systematic review.’ 2023.
-
[4] PMC / National Institutes of Health. Burnout impact on medical errors and malpractice. Ibid.
-
[5] Diagnostic Imaging. ‘Current Perspectives on Radiology Workforce Issues and Potential Solutions.’ December 2025.
-
[6] Healthcare IT News. ‘Radiology staff report alarming levels of stress & burnout in new Philips study.’
-
[7] Nature / npj Health Systems. ‘AI solutions to the radiology workforce shortage.’ May 2025.
Tags:
radiology workflow optimization, radiology clinical efficiency, radiology workflow management, radiology burnout solutions, display calibration in radiology, diagnostic imaging workflow, radiology productivity improvement, medical imaging workflow optimization, radiology quality assurance, radiology technology efficiency